当前位置:EASL-欧洲肝脏研究协会年会 » 正文
[重磅]相似的疗效和更好的肾脏骨骼安全性——磷丙替诺福韦(TAF)在慢性乙型肝炎中的应用价值
—— 作者: 时间:2017-04-23 05:31:01 阅读数:
1857

2017年4月20日,欧洲肝脏研究学会(EASL)发布了2017版最新乙型肝炎管理指南,其中对于初治慢乙肝患者的一线首选核苷(酸)类似物(NA)治疗方案,在原有的富马酸替诺福韦二吡呋酯(TDF)和恩替卡韦(ETV)之外,EASL指南增加了磷丙替诺福韦(tenofovir alafenamide,TAF)。
由于慢性乙型肝炎(简称慢乙肝)的主要治疗目标是延缓和减少疾病进展和肝功能衰竭,肝硬化失代偿,肝细胞癌(HCC)及其他并发症的发生,从而改善生存和生活质量,长期抑制HBV DNA水平成为当前治疗策略的主要终点。根据更新的指南,在NA长期治疗中应选择安全性得到优化的方案,特别是对于合并疾病增加的老年慢乙肝患者。指南还推荐,对于患有肾脏疾病或骨骼疾病和/或有发生上述疾病风险的患者,特别是曾经有过核苷(nucleoside)类似物暴露的人群,应首选TAF治疗。
TAF已在美国、欧洲和日本等地获批,主要基于两项III期、随机双盲,以TDF为活性对照的非劣效性研究(108研究和110研究)。这两项研究的96周结果于4月20日在本次EASL大会(ILC2017)上公布,而TAF在中国的临床试验也正在开展中(尚未在我国获得批准上市)。下文带您详细了解在美国肝病学会年会(AASLD)和EASL等顶级肝病学术会议上报道的最新临床研究数据。
慢乙肝的疾病负担和当前治疗推荐
目前全球约有2.4亿慢性HBV感染者,如果不治疗,其中约1/4将死于肝硬化、肝衰竭和肝细胞癌(HCC)。每年约有65万人死于慢乙肝及相关并发症。我国约有慢性HBV感染者9300万人,其中慢乙肝患者约2000万例。
目前已达成共识,慢乙肝的治疗目标是减轻肝细胞炎性坏死及肝纤维化,延缓和减少肝功能衰竭、肝硬化失代偿、HCC及其他并发症的发生,从而改善患者的生活质量和生存。而要实现上述目标,需要最大限度地长期抑制HBV复制。初治患者在使用NA治疗时,应首选强效高耐药屏障药物,如TDF、ETV以及最新被写入EASL指南的TAF。
以TDF为例,治疗8年的意向性治疗分析显示,分别有58%的HBeAg阳性患者和75%的HBeAg阴性患者的HBV DNA低于检测下限(<69 IU/mL),而根据on-treatment分析,TDF治疗8年,98%的HBeAg阳性患者和99.6%的HBeAg阴性患者实现了病毒学应答,并且未检测到TDF相关耐药。TDF的整体耐受性和安全性很好,治疗8年时,2.2%的患者出现血肌酐升高≥0.5 mg/dL,1.7%的患者有过一过性低磷血症。
临床实践中,尽管在TDF治疗期间可能有少数患者出现肾脏事件和骨质疏松,不过据分析,很多相关事件可能与不规范的临床实践,以及不依从指南推荐的给药方案和说明书中列出的其他注意事项等有关,如治疗前未对患者的病史和治疗史进行详细评估,对患者肾脏和骨骼状况及相关风险因素不了解,治疗时也未根据估算肾小球滤过率等指标调整用药剂量等。
由于慢乙肝患者逐渐变老,合并症会越来越多。一项来自1334例慢乙肝患者的队列研究显示,在总体人群中,慢性肾病(CKD)的发生率为7.2%,在年龄超过65岁的患者中发生率为为14%,合并高血压/糖尿病的患者比例更是达到了25%。加之慢乙肝患者需要长期甚至是无限期服药,所以对抗病毒药物的安全性要求越来越高。
96周数据显示TAF的强效抗病毒和改善肾脏、骨骼安全标志物
TAF与TDF均为替诺福韦(TFV)的前药(图1)。TAF在血浆中的稳定性更好,血浆中的半衰期为90 min(TDF为0.4 min),相比TDF更能有效地将TFV送达到肝细胞。在肝细胞中,TAF被分解成为有活性的代谢产物,二磷酸替诺福韦。要达到相同活性代谢产物浓度所需的给药剂量,TAF仅为TDF的约1/10(25 mg vs 300 mg),这使得TFV在血液中的系统暴露量减少了89%。

图1. 磷丙替诺福韦概况
108研究和110研究的设计方案相同。前者纳入了425例HBeAg阴性慢乙肝患者,后者纳入了873例HBeAg阳性慢乙肝患者。患者按2∶1的比例随机接受TAF(25 mg,QD)或TDF(300 mg,QD)治疗。本次会议上,意大利比萨大学Brunetto教授和英国国王学院医院Agarwal教授分别报告了TAF治疗HBeAg阴性慢乙肝和HBeAg阳性慢乙肝96周的疗效和安全性结果(摘要号:PS-042和FRI-153)。
TAF治疗慢乙肝96周维持高效
之前48周的数据显示,TAF的抗病毒疗效不劣于TDF。治疗48周时,HBeAg阴性人群实现HBV DNA水平<29 IU/mL的患者比例在TAF组和TDF组分别为94.0%和92.9%,HBeAg阳性人群的应答比例在TAF组和TDF组分别为63.9%和66.8%(P=0.25)。
治疗96周,HBeAg阴性人群的病毒学应答率在TAF组和TDF组分别为90%和91%(校正后的差异为0.6%,P=0.84);HBeAg阳性人群的病毒学应答率在TAF组和TDF组分别为73%和75%(校正后的差异为2.2%,P=0.47)。两组的病毒学应答数据如图2所示。

图2. TAF与TDF治疗慢乙肝患者48周和96周的病毒学应答(HBV DNA<29 IU/mL)
TAF组有更多的患者实现血清ALT复常,按中心实验室标准,96周时ALT复常率在HBeAg阴性人群为81% vs. 71%(P=0.035),在HBeAg阳性人群为75%vs.68%(P=0.017)。HBeAg清除率在两组相似。在108研究中(HBeAg阴性人群)TAF组有1例患者出现HBsAg清除并在治疗80周时出现血清学转换,在110研究中(HBeAg阳性人群)TAF组有7例患者出现HBsAg清除并有6例实现血清学转换,TDF组有4例患者出现HBsAg清除但没有患者实现血清学转换。
TDF换用TAF后骨骼和肾脏安全性数据改善
之前48周的数据显示,TAF的骨骼和肾脏的安全标志物与TDF相比有所改善,这个效果持续到了治疗96周。与TDF相比,TAF组患者96周的髋关节和脊柱的骨矿物质密度(BMD)较基线的下降更少,eGFR的下降更少,肾小管标志物的变化更少(图3、表1)。两组的不良事件发生率相似,因不良事件停药和3~4级严重不良事件的发生率低。根据TAF产品说明书,TAF最常见的不良反应(发生率≥5%)为头痛、腹痛、乏力、咳嗽、恶心和后背疼痛。

图3. TAF和TDF治疗期间患者髋关节(hip)和脊柱(spine)骨矿物质密度的变化
(上图:HBeAg阴性患者,下图:HBeAg阳性患者;可见TAF组的BMD下降更少,而且这个差异在96周更加明显)
表1. TAF和TDF治疗期间患者肾功能指标的变化

TDF换用TAF后骨骼和肾脏安全性数据改善
我国香港中文大学陈力元教授在会议上报告了上述两项研究中,完成双盲阶段研究的患者换用TAF治疗24周,其肾脏和骨骼参数的变化和病毒抑制效果的维持(摘要号:PS-041)。截止分析时,分别有200例HBeAg阴性患者和340例HBeAg阳性患者完成了96周的治疗并换用TAF开放标签治疗。
结果显示,TDF换用TAF治疗24周(n=117),患者的肌酐清除率显著改善,变化均值为增加2.43 mL/min(P=0.02),TAF继续治疗的患者的肌酐清除率维持稳定(图4)。同样,在BMD方面,TDF换用TAF治疗24周后也表现出显著改善,与96周相比P<0.001(图5),TAF继续治疗组则维持稳定。病毒学抑制方面,两个人群都表现出持续的强效病毒抑制,HBeAg阴性人群为97%~99%,HBeAg阳性人群为80%~83%。

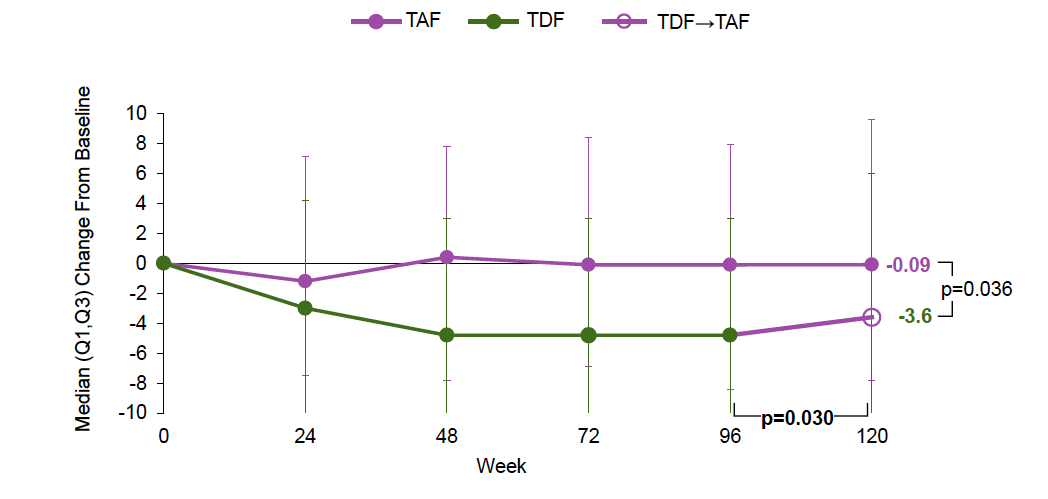
图4. TDF换用TAF治疗24周的肌酐清除率变化

图5. TDF换用TAF治疗24周的骨密度变化
总结
TAF在维持强效抑制病毒作用的同时,表现出更高的ALT复常率,HBeAg血清学转换率更高,以及对肾脏和骨骼安全性指标的影响更少。此外在临床试验中,TDF换用TAF治疗仅24周,患者的BMD和肌酐清除率表现出改善。未来将会有更多的长期数据,或将为如何实现最佳的长期安全管理提供更多信息。我们期待未来有更多TAF在初治以及经治人群中的应用数据,帮助临床制订更有效和更安全的治疗策略。
The above posting is sponsored by Gilead Sciences to support scientific and medical education, and with non-promotional intent. The content was reviewed prior to publication by Gilead Sciences.
以上文章由Gilead Sciences赞助以支持科学及医学教育,且无推广意图。文章内容发布前已经过Gilead Sciences审阅。
[Feature] Similar efficacy and improved kidney and bone safety markers—the value of TAF in treating chronic hepatitis B
The European Association for the Study of the Liver (EASL) released an updated Clinical Practice Guideline on the management of hepatitis B virus (HBV) infection on April 20th, 2017, and in addition to tenofovir disoproxil fumarate (TDF) and entecavir (ETV), tenofovir alafenamide (TAF) was added as a first-line recommended regimen.
Since the main goal for chronic hepatitis B (CHB) treatment is to improve survival and quality of life by preventing disease progression and HCC development, the long-term suppression of HBV DNA levels is the main endpoint of current treatment strategies. According to the updated guideline, an optimized safety profile of a long-term nucleos(t)ide analogue (NA) therapy should be used, particularly in an ageing CHB population with increasing comorbidities. The guidelines recommend TAF as a preferred choice for patients at risk of development and/or with underlying renal or bone disease, especially those with previous exposure to nucleoside analogue.
TAF has been approved in the U.S., Europe, and Japan, mainly based on two randomized double-blinded, non-inferiority phase 3 studies that had TDF as active control (Studies 108 and 110). The 96-week results of these two studies were also announced on Apr. 20th at this year’s EASL conference. TAF clinical studies are being implemented in China, where it has not approved. Next, we will introduce you to clinical study data recently presented at leading scientific congresses for liver disease, including AASLD and EASL.
The burden of the chronic hepatitis B disease and the current recommended therapies
Currently there are about 240 million chronic HBV infected patients globally, and if not treated, about 1/4 of them will die from cirrhosis, liver failure, and hepatocellular cancer (HCC). Each year, there are about 650 thousand people die from Hepatitis B and its related complications. Our country has about 93 million people with chronic HBV infection, and among them about 20 million are chronic hepatitis B (CHB) patients.
It is a common view that the goal of treating CHB is to reduce liver cell inflammatory necrosis and liver fibrosis, delay and reduce the incidence of liver failure, decompensated cirrhosis, HCC, and other complications, in order to improve patients’ quality of life and their survival rate. To achieve the above goal, we need to maximize the inhibition of HBV duplication on the long-term. When treating naive patients with NA, we should first consider the drugs that are highly potent and with a high barrier to resistance, such as TDF, EVT, and TAF that has been listed into EASL guideline recently.
Regarding TDF, the 8-year intention-to-treat data shows that the HBV DNA is lower than the detection limit (<69 IUs/mL) for 58% of the HBeAg-positive patients and 75% of the HBeAg-negative patients, and according to on-treatment data, 98% HBeAg-positive patients and 99.6% HBeAg-negative patients have reached virological response after 8-year treatment of TDF and no drug resistance is found. The overall tolerance and safety profile of TDF is very good. However, by the end of the 8th year, 2.2% subjects had serum creatinine ≥0.5 mg/dL from the baseline and 1.7% had transient hypophosphatemia.
Although there were kidney and bone related problems happened to several patients during TDF treatment, according to analysis, many incidence might be associated with improper clinical practices as well as failure to adhere to recommended dosing guidelines and other precautions listed in the product label. For instance, the lack of detailed assessment of patient’s disease history and treatment history prior to their treatment, the lack of understanding of patient’s kidney and bone conditions as well as related risk factors, and the dosage was not adjusted according to indicators such as the estimated infiltration rate of glomerulus during treatment.
Meanwhile, complications will develop as chronic Hepatitis B patients grow older. A cohort study that enrolled 1334 chronic Hepatitis B patients indicates that the prevalence rate of CKD is 7.2% in all patients, while for patients aged over 65, the CKD rate is 14% and hypertension/diabetes complication rate has reached to 25%. In addition, chronic Hepatitis B patients require long-term and even infinite treatments, so they would require continually improved safety profile for DAA drugs.
The 96-week data showing anti-virus potency of TAF and its improved kidney and bone safety markers
Both TAF and TDF are the prodrug of Tenofovir (the difference between the two is shown in Figure 1). TAF is more stable in plasma with a half-life of 90 min (the half-life of TDF is 0.4 min), and can deliver TFV to hepatocytes more effectively comparing to TDF. In hepatocytes, TAF is broken down into active metabolite, Tenofovir Diphosphate. To produce the same concentration of the active metabolite, the dosage needed for TAF is only about 1/10 of that needed for TDF (25 mg versus 300 mg), resulting an 89% reduction of TFV exposure in the blood system.
Figure 1. Introduction of tenofovir alafenamide(TAF)
The study designs of study 108 and 110 are the same. The former enrolled 425 HBeAg-negative patients and the latter enrolled 873 HBeAg-positive patients. The patients randomly received treatment with TAF (25mg, QD) or TDF (300mg, QD) at a ratio of 2:1. At this year’s conference, professor Brunetto from University of Pisa in Italy and professor Agarwal from King's College London School of Medicine in UK respectively reported the efficacy and safety of the TAF 96-week treatment for HBeAg-negative patients and HBeAg-positive patients (abstract’s serial numbers: PS-042 and FRI-153).
Sustained efficacy of TAF in treating CHB for 96 weeks
The previous 48-week data shows that TAF’s anti-virus efficacy is comparable to that of TDF. After 48 weeks of treatment, the percentage of HBeAg-negative patients whose HBV DNA level is <29 IU/ml is 94.0% and 92.9% in the TAF group and the TDF group respectively, and the response rate of the HBeAg-positive patients is 63.9% and 66.8% (P=0.25) in the TAF group and the TDF group respectively.
After 96 weeks of treatment, the virologic response rate of the HBeAg-negative patients is 90% and 91% in the TAF group and the TDF group respectively (the difference after calibration is 0.6%, p=0.84); the virologic response rate of the HBeAg-positive patients is 73% and 75% in the TAF group and the TDF group respectively (the difference after calibration is 2.2%, p=0.47). The virologic response data of the two groups is shown in Figure 2.
Figure 2. The SVR of TAF and TDF Treating Chronic Hepatitis B Patients for 48 weeks and 96 weeks (HBV<29 IU/mL)
There are more patients whose serum ALT level is back to normal in the TAF group than that in the TDF group – according the research standard, the percentage of patients with ALT back to normal in 96 weeks is 81% versus 71% (P=0.035) among the HBeAg-negative patients and 75% versus 68% (P=0.017) among the HBeAg-positive patients. HBeAg clearance rates are similar in both groups. In the TAF group, 1 HBeAg-negative patient showed HBeAg clearance and had seroconversion after 80 weeks of treatment.
Improved safety markers for bone and kidney during 96 weeks of TAF treatment for CHB
The previous 48-week data shows that bone and kidney safety markers were improved for TAF as compared to TDF, and this improvement lasts to the 96th week of the treatment. Compared to TDF, the decline of bone mineral density (BMD) of the hip joint and spine from the baseline was smaller, the decline of eGFR was smaller, and the change in the markers of kidney tubules was also smaller for patients in TAF 96 weeks of treatment group (see chart 1). The adverse rates are similar for both groups, the withdrawal rate due to adverse events and the incident rate of level 3-4 severe adverse events are low. According to the product instruction of TAF, common adverse events (incident rate ≥5%) including headache, abdominal pain, fatigue, cough, nausea, back pain.
Figure 3. The BMD Changes of Spine and Hip during TAF and TDF Treatment
(Above: HBeAg-negative patients, Blow: HBeAg-positive patients; The BMD decrease is smaller in TAF group, and the difference becomes distinct in week-96)
The data of bone and kidney safety is improved after using TAF to replace TDF
At the EASL conference, Professor Henry Chan from Chinese University of Hong Kong reported the change of kidney and bone parameters and the retainment of virus inhibition for patients in the above two studies to whom TAF was used to replace TDF after the double-blinded 24 weeks treatment (abstract serial number: PS-041). As of the time when this analysis was conducted, 200 HBeAg-negative patients and 340 HBeAg-positive patients completed 96 weeks of treatment and TAF was used to replace TDF for open-label treatment.
The result shows that, after using TAF to replace TDF for 24 weeks of treatment (n=117), the creatinine clearance of the patients was significantly improved, with an average increase of 2.43ml/min (P=0.02), and the creatinine clearance of the patients who previously receiving TAF treatment remained stable (Figure 4). Similarly, after using TAF to replace TDF for 24 weeks, patient’s BMD was also significantly improved, with p <0.001 comparing to 96 weeks (Figure 5), and the BMD of those previously receiving TAF treatment remained stable. In terms of virologic control, both groups demonstrated sustained strong virologic inhibition - the percentage was 97%-99% for HBeAg-negative patients and 80%-83% for HBeAg-positive patients.
Figure 4. The change of creatinine clearance rate in 24 weeks after switching TDF to TAF
Figure 5. The change of BMD in 24 weeks after switching TDF to TAF
Conclusion
While maintaining virologic inhibition, TAF demonstrated a higher ALT recovery rate, a higher HBeAg seroconversion rate, as well as a less impact on kidney and bone safety markers. In addition, after using TAF to replace TDF for 24 weeks of treatment, patients’ BMD and creatinine clearance showed improvement in clinical trials. Additional long-term data is anticipated in the future which may provide further information on how best to achieve long-term safety management. We are expecting to see more TAF data in naive patients as well as previously treated patients in the future, to help us designing a more effective and safer clinical practice strategy.
标签:
传真
现场快报
乙肝
发表评论
全部评论